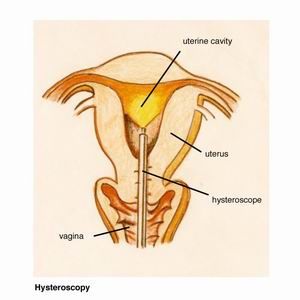
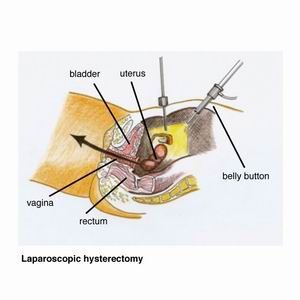
What is laparoscopy? Laparoscopy is an operation which allows the surgeon to see and operate on the organs inside the pelvis and abdomen (belly). The pelvis is the basin-shaped cavity at the lower end of the body formed by the left and right hip bones and includes the genital region. A small 5 to 10 mm incision (cut) is made in the belly button through which the laparoscope (this is like a telescope) is inserted with a video camera attached. Further instruments are inserted through another three little cuts in the lower abdomen.  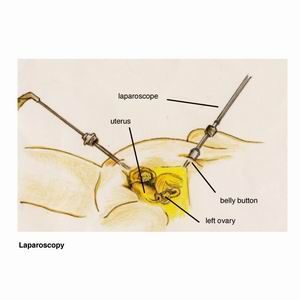 Carbon dioxide gas is used to distend the abdomen. This is inserted through a needle via the belly button, but this may not be possible in all cases. Therefore a larger incision through the belly button may be required or a needle may be placed just below the left ribcage. At the time of the laparoscopy an instrument (uterine elevator) is inserted via the vagina into the uterus. This allows the surgeon to lift and move the uterus which is required for the laparoscopy. A video and/or photos will be taken during the operation and used to show you what was seen and done. Dr Varol will send you a copy of the operation report together with the photos taken before and after surgery. Laparoscopy has many advantages over open surgery, small incisions versus a bigger cut, like we do for a caesarean section, is one of them. 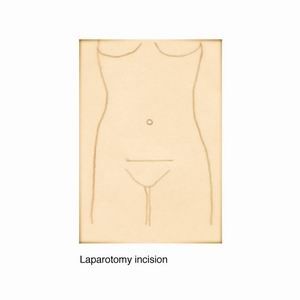 Laparoscopy's advantages over open surgery are:
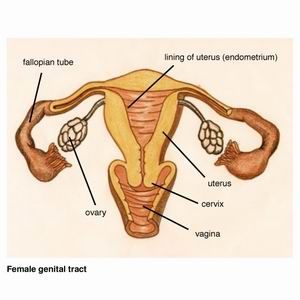
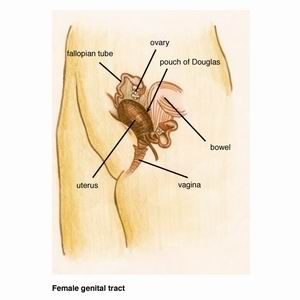
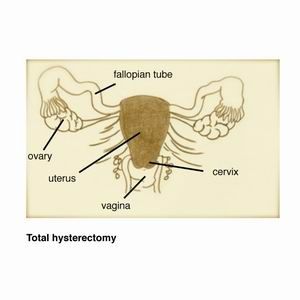
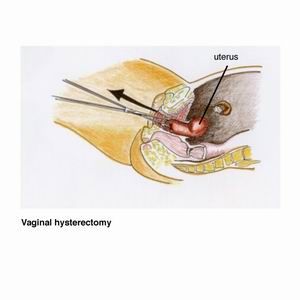
A laparoscopy is done under a general anaesthetic, so you are asleep for the operation. Some of the reasons to perform a laparoscopy are the following: Endometriosis The surgeon is able to remove endometriosis and free adhesions. An adhesion refers to tissues or organs that are stuck together, when naturally they should be apart. Hysterectomy A hysterectomy (removal of the uterus) can be detached from the surrounding tissue with the instruments that are inserted through the little laparoscopy incisions (cuts) in the tummy. The uterus is then removed through the vagina, thus avoiding the need to make a large incision. This operation usually a three day stay in hospital and most patients return to full activity within three weeks. Ectopic Pregnancy An ectopic pregnancy is a pregnancy that occurs outside the uterus, usually in the fallopian tubes. Three incisions are made in the abdomen and the fallopian tube is removed at laparoscopy. Fibroid Depending on the size and position of fibroids, they can be removed at laparoscopy without needing to make a larger incision in the abdomen. Investigation of infertility and pelvic pain Some of the causes of infertility and pelvic pain can be treated successfully at laparoscopy, such as endometriosis and adhesions. Diet before your laparoscopy You will be given a diet form which explains in details what you can and cannot eat before your laparoscopy. This is very important as your bowels need to be empty for the operation. If you have endometriosis or other disease that is near or on the bowel, then this can only be removed if the bowel is empty. If the operation is scheduled for the afternoon at Royal Prince Alfred Hospital, you need to stop eating and drinking at 6 am the morning of your surgery. Medication It is important to continue to take your usual medications such as those for high blood pressure, diabetes and the oral contraceptive pill. If you have been taken non steroidal anti-inflammatory medications such as aspirin, Ponstan, Nurufen, Naprogesic etc, you should stop them 14 days before your operation. You may take tablets that contain paracetamol and codeine such as Panadol, Panadeine or Panadeine Forte for pain relief. Hospital Stay You will be admitted to The Perioperative Unit at Royal Prince Alfred Hospital for one night if you are having a laparoscopy. This is located on the third floor of the hospital. If you are admitted for a hysterectomy or an open surgery (laparotomy), you will be shown to one of the wards in the hospital and your hospital stay will take a few days. You will be taken to the operating theaters in a bed and the anaesthetist will see you and explain what is going to happen before you fall asleep. He will put a cannula into one of the veins in your hand or arm. He will give you some medication to make you feel relaxed and you will then be taken into the operating room. The anaesthetist will place a mask on your face for you to take some deep breaths of oxygen. He will then administer anaesthetic drugs through the drip in your arm and you will fall asleep. When you wake up, you will find yourself in the Recovery Room where there is a nurse who will look after you. You will be given drugs to keep you comfortable and pain free. After half an hour to an hour you will return to your initial ward. Dr Varol will see you after the operation and explain the surgery to you, what was found and what was done. You will also be seen the next morning before you go home. After Your Operation You will need someone to look after you for about two to three days when you come home. In general you will need one week off from week. Some women may need two weeks recovery at home. Wounds In general you will have 4 small wounds in your tummy which have dressings on them. There will be a little bit of blood underneath the dressings which is normal. They are waterproof and you can take a shower as usual. Take the dressings off 4 days after your operation, i.e. if your operation was on Tuesday at Royal Prince Alfred Hospital, you should take them off on Saturday. In general there will be a stitch underneath the skin in the belly button wound which will dissolve by itself. The other wounds won't have a stitch but steri strips which are strong sticky tapes for wounds. Sometimes a stitch may need to be placed in those wounds as well and they usually dissolve by themselves. If stitches need to be removed, Dr Varol will inform you after the operation. Pain Because the wounds from laparoscopy are very small, they heal fairly quickly with minimal scarring. There will be some pain from the operation and you will be given a script for Panadeine Forte which you will need for a few days. Every day you should feel better than the previous day. If you suddenly feel worse or have more pain, please contact Dr Varol. You can contact her 24 hours a day. Diet It is best to have a healthy diet after your operation with fruits, vegetables & lean meats. You should avoid fatty & fried foods. It's easy to become constipated after an operation, so have plenty of fluid to drinks & eat some fruits. Fruits that are particularly good for constipation are prunes and guavas. You may need to take some extra medication such as Metamucil or coloxyl and senna tablets. If you had part of your bowel removed, your diet will be different and Dr Varol will explain that to you. In general she will want you to be on a fluid diet for a few days before you start on solid foods. Work In general you need one week off from work after a laparoscopy. Some women may need two weeks, depending on how you are recovering and your type of work. Driving As with any procedure that requires a general anaesthetic, you must not drive for the first 24 hours after discharge from hospital. A responsible adult needs to pick you up from hospital and take you home. If you had a hysterectomy or an open operation, you should not drive for four to six weeks. Return to Normal Activities Recovery time depends on the individual and the type of operation you have had. In general you will find it too uncomfortable to do any kind of heavy work or exercise such as vacuuming, carrying heavy things, aerobics etc for a few weeks. The general rule is that if an activity makes you feel tired or gives you pain or discomfort, you should not do it. Dr Varol will let you know how long it will take you to get back to normal activity. Sex After a laparoscopy you may resume sexual activity when you feel comfortable enough and there is no more bleeding from the vagina. That usually takes one to two weeks. If you had a hysterectomy, the stitches in the top of the vagina need to heal before you can have sex again. That takes about four to six weeks. Complications of laparoscopic surgery Please see the section under ?Consent for Laparoscopic Surgery? for the details of the possible complications with laparoscopic surgery. Follow up appointment In general you should ring Dr Varol's practice to make an appointment for four weeks after your operation. If you have any problems, concerns or questions, please ring her as per details below. Dr Varol's contacts details office hours : Ring her practice on 9223 7200 after hours : Ring Royal Prince Alfred Hospital (RPAH) on 9515 6111 and ask switchboard to page Dr Varol. Leave your name and number and Dr Varol will call you back promptly. If there is a problem, ask switchboard to put you through to her mobile number. |

|

|